
If epidemiologists and Public Health specialists are right, Canada has just about reached the peak – or at least a plateau – on the COVID-19 curve. How long we stay at the peak before coasting down the other side is uncertain. New cases are still being reported in large numbers but they have tended to level out rather than increase exponentially. A significant number of deaths are also still occurring, especially associated with Long Term Care facilities, but these, too, are anticipated to start to decline in the next couple of weeks.
When I wrote about this in mid-March, the fear was that we would be overwhelmed with a surge in COVID-19 infections that would inundate our Health Care Facilities and hospitals with patients requiring intensive care. We were cautioned that we must “flatten the curve” and with Public Health guidance, we significantly changed our social interaction with others and washed our hands until they are raw. This strategy seems to have worked as hoped.
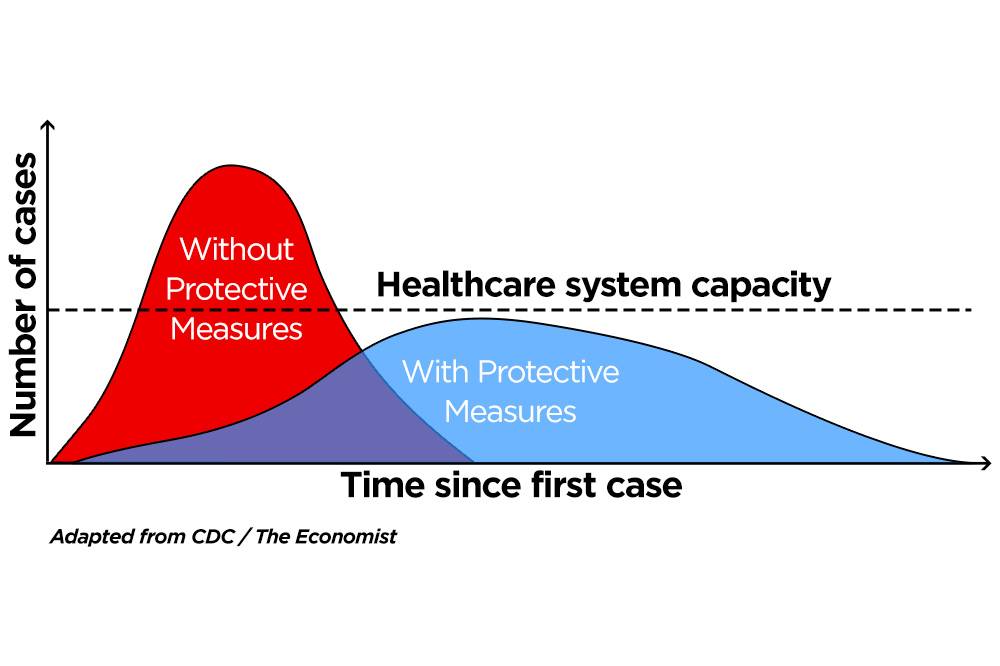
We must bear in mind, however, that we are flattening the curve, not eliminating it all together. Yet. The downward curve will be very gradual and prolonged. COVID will linger for quite some time and there will always be the threat that if we lighten up our precautions too quickly the curve will bump up where we don’t want it to be.
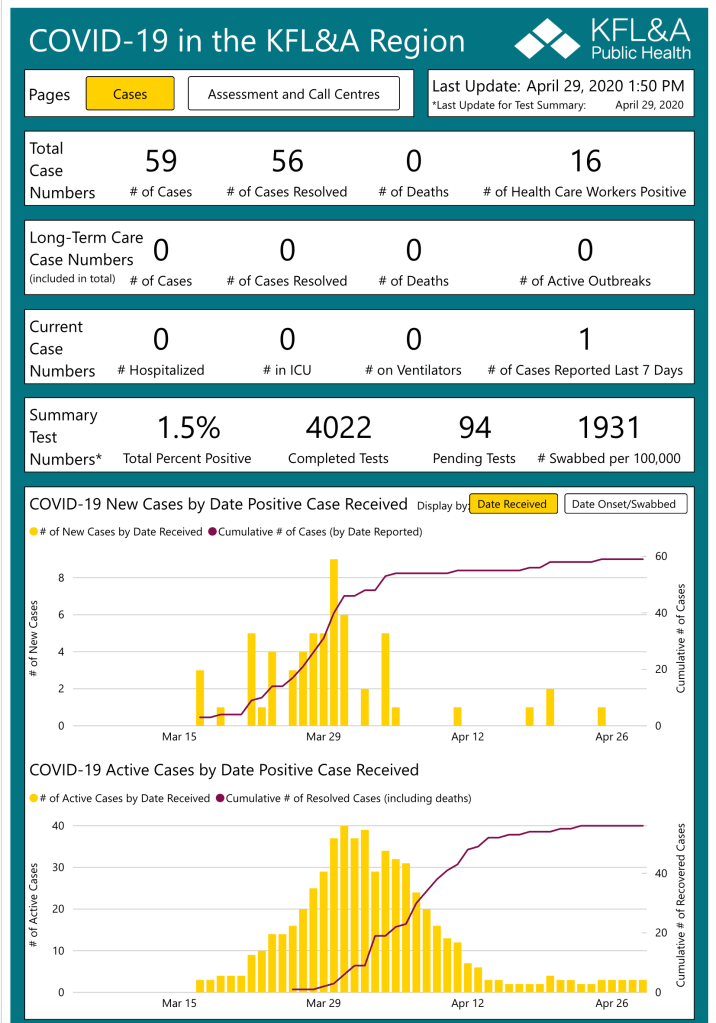
In Kingston, Ontario, where I live, we have been especially fortunate to have avoided the anticipated huge peaks and potential overwhelming surge on our Health Care facilities. The KFLA Health Unit, serving a population of about 215,000, reports today that there have been a total of 59 confirmed cases with 56 of them already declared “resolved”. Our health unit has recorded no COVID-19 deaths. No COVID-19 patients are currently in our ICU or on a ventilator. In the last three weeks there have been only four newly-confirmed cases. Thanks to both good luck and preemptive precautions taken by our local Public Health Unit, our Long Term Care facilities have, so far, remained safe with no outbreaks. This is indeed a great relief for our community. You can see for yourself in the image at the end of this post, how our local curve has remained flat for several days.
This good news does come with a bit of a snag, however. Because our community has been so spared of a significant outbreak, it means that most of us are COVID-19-susceptible. The challenge becomes how we can start to relax our restrictions but not find ourselves at square one again because very little has actually changed about our community in terms of COVID-19 vulnerability. As long as we remain somewhat cloistered as a community, our risks of infection are lower than many other areas that have been more heavily infected. But how long can we remain isolated as people start to travel a bit more widely to visit family or students return to Kingston or folks take a bit of a vacation in the summer outside our area?
The Ontario government has published a scheme whereby things might gradually open up but the timing of reducing restrictions will be entirely dependent on what is happening in terms of infection rates, hospitalizations and deaths. Realistically, it will take a long, long, time to return to any semblance of normal. And the normal that we return to will inevitably be different from our past. The physical distancing thing will certainly remain a standard for some time. It will affect the way we shop, interact with friends, travel and celebrate together. Group activities will be curtailed for months to come.
There is still a lot that we don’t know about this virus. We will need more widespread NP swab testing to identify the presence of virus. When we test more broadly, we will be able to identify earlier the people who might be infected and thereby infectious to others. If we quarantine those people and actively contact trace to find anyone who might have had interaction with them and then test and isolate those people, we will reduce exposure to others within the community. We know that there is a significant number of people who exhibit no symptoms and yet are infected and able to spread the virus. We need to be more aggressive with testing to identify as many as we can so the transmission to others is reduced.
Eventually antibody testing to determine the presence of both recently and more remotely acquired antibodies that hopefully will result in immunity will give us a better sense of how widespread asymptomatic or mildly symptomatic infections have been.
I anticipate that some medical management will soon be determined to be available to those who are more acutely ill. This would really help to manage the severely ill and reduce the strain on hospital resources. We have not found this treatment yet but I am certain that eventually we will discover an effective management strategy.
The ultimate fix that will allow us to return to “normal” will be if and when an effective, safe vaccine is developed and made widely available to people throughout the world. We know that vaccination works. Consider, for example, what immunization has done to squash Smallpox, Polio, Tetanus, Measles. Getting it right is important, however, so that we know that it is safe and effective. Combined with antibody testing, this might be the ultimate “Get out of jail free” card we await.
I have spoken to a lot of people who are wondering if the cough and fever that they had in January was actually COVID-19. Although we know that this COVID-19 virus was probably circulating, undetected, weeks before it was first identified in labs, it is probably more likely that most of those folks with “flu” early in the year were suffering from another viral illness. Acute Respiratory Infections caused by a number of agents give similar clinical pictures. The only way to find out how many of those January coughs were COVID-19 will be when the antibody test is available for widespread use.
In the mid 1980’s when HIV was ravaging various segments of our society and decimating African communities, we talked about ‘safe’ sex. Eventually we realized that no sex was 100% safe so we changed the terminology to ‘safer’ sex. I think we will need to think similarly about COVID-19. Until a large percentage of the entire world has developed immunity, this virus will be present and we will have to do what we can to minimize our own risks and limit spread in our community. It won’t be perfect, but with careful hand washing, limited close contacts, changes to the way that we gather in groups, physical distancing where practical, testing, contact tracing and eventual immunization, we will be able to cautiously inch forward to arrive at a new normal. The world has encountered plagues and epidemics and pandemics before and survived. We will too. But it will take a long time to get there and many things will have changed irrevocably in the meantime.
John A. Geddes MSc MD CCFP
