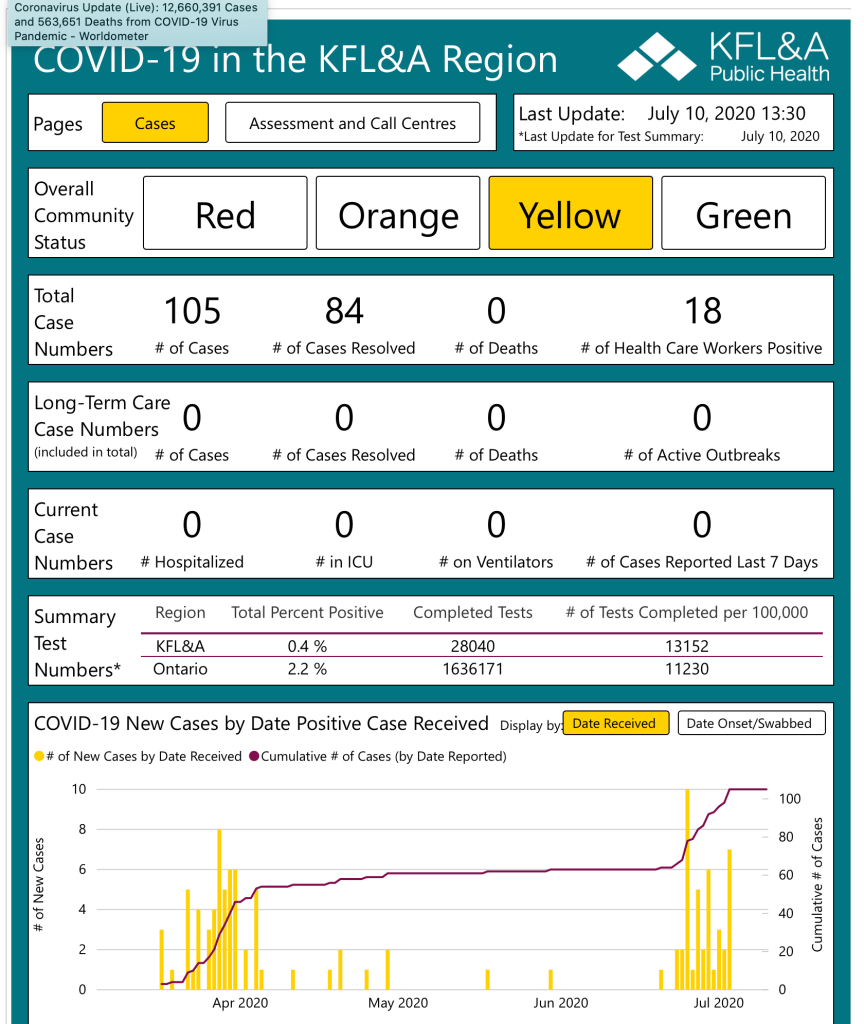
The COVID-19 news, both globally and in Ontario, has been discouraging in the past few weeks. In Kingston, we have done remarkably well throughout the pandemic but new cases are currently occurring at greater daily counts than our usual and today we have the highest active case count that we have had since all this began. A recent B117 outbreak involving a local construction site where there were “workers from multiple jurisdictions” will probably impact our community for some time as it can spread to close contact family members.
Is there any light at the end of this seemingly endless tunnel?
Unfortunately, Canadians were a bit smug about our case numbers when comparing them to other parts of the world, including the U.S.A. and U.K. We became complacent about continuing the recommended Public Health measures that have been advised since the beginning of the pandemic. We were tired of the restrictions and our Health Care System was managing, so we let down our guard. Although we ought to have heeded the February warnings about variants on the horizon that had caused high caseloads in the UK, Brazil and South Africa, we ignored those foreboding predictions and continued to be open for business with minimal personal or business restrictions. We responded too late and too little. Can we find any hope in looking at how other countries have emerged from this dilemma that is pushing our provincial health care systems to the breaking point?
Bear with me as I throw a few graphs your way. My story ends with a possible positive outcome if that will encourage you to read on. Not surprisingly, it appears that successful reduction in COVID-19 case numbers relates directly to vaccination rates and countries following disciplined public health restrictions.
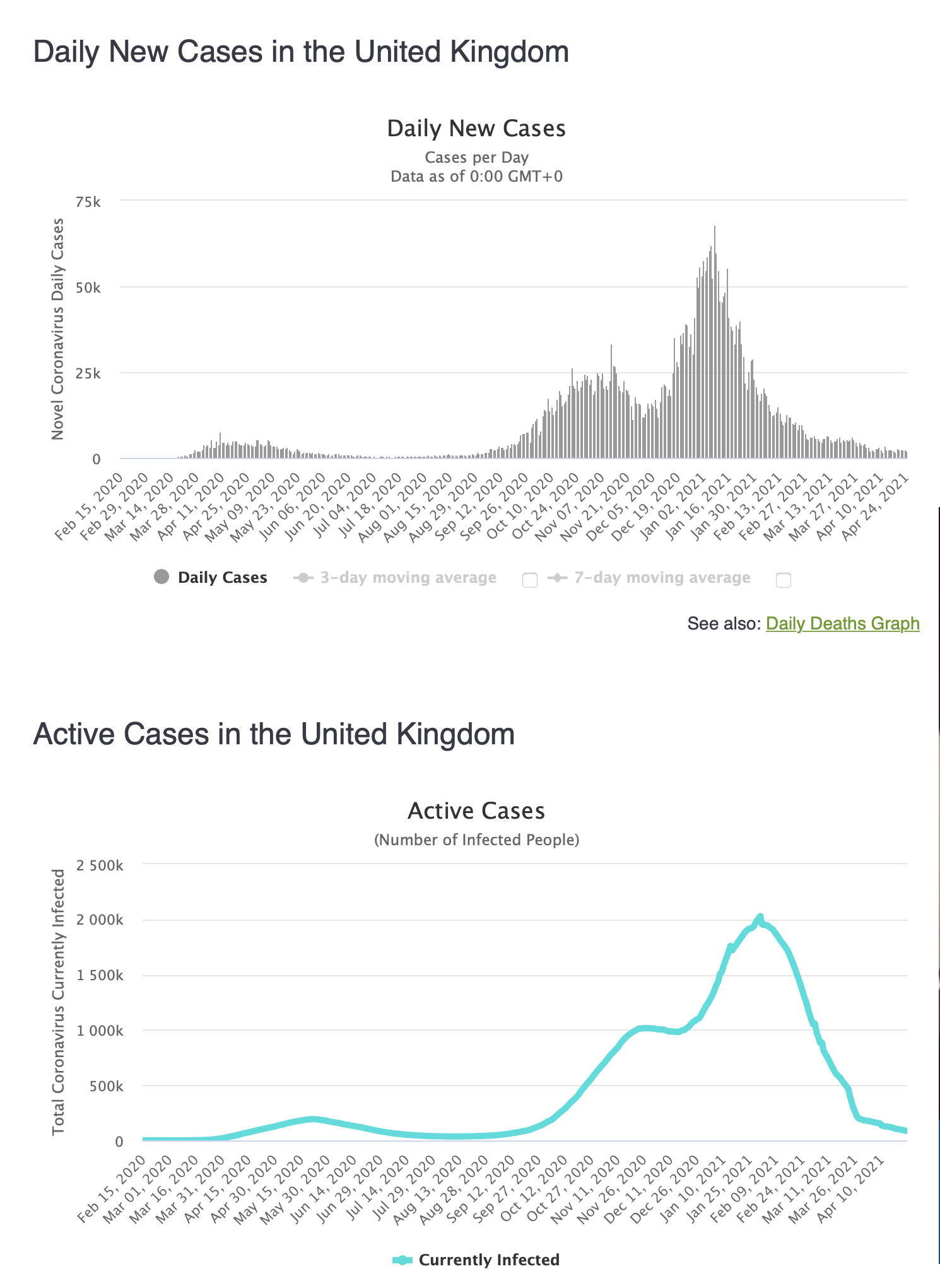
Not long ago the UK was in bad shape with COVID-19. The new B117 variant that is plaguing us now had gained hold there and was causing surging in caseloads that peaked in January They locked down and vaccinated extensively, mainly using the Astra Zeneca vaccine. What happened? Their number of new cases has been dropping continuously. Today they report that over 50% of their population has had at least one dose of vaccine. Persistence with lockdown restrictions and a good uptake of vaccinations seems to have helped to turn the COVID corner for the UK. They now have a graduated schedule of return to “normal” that will slowly open things up, stretching until late June.
Is this just a fluke? We can also look at Israel’s experience where the combination of lockdown and vaccination (mostly Pfizer) also had a significant effect. In January, Israel was also experiencing a serious second wave of COVID-19. However, they got an early start with aggressive vaccination while imposing significant restrictions including mandatory mask-wearing outdoors, school closures and restricted travel into the country . Now their numbers are very low and they are starting to open up and have reduced restrictions. Last week Israel reported their first day in 10 months without a COVID-related death in the country. They are being cautious as they slowly reopen but it appears that things are getting back to “Normal”.

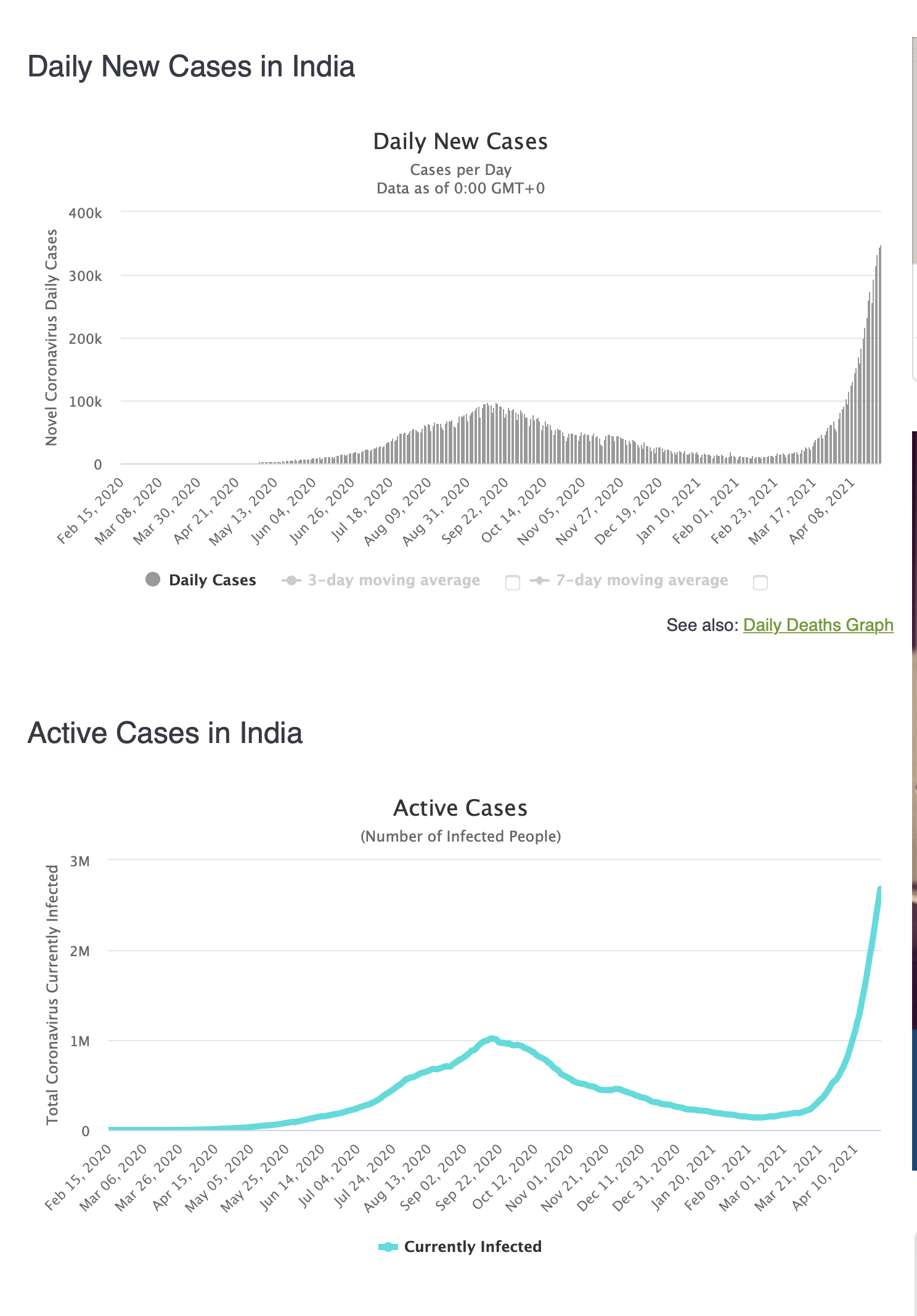
India, with a huge population, had a false sense of security when numbers started to abate early in 2021 and led to them quickly reopening the country to things like large social and religious gatherings and sporting events. Even though they produce vaccine, some of which has been sold to Canada, their own programme has been slow to develop. They are now faced with a new variant and in the past few days their numbers have been astronomical and the death toll is staggering. The current surge in cases and deaths is having an absolutely devastating effect in India that will be felt around the world. The COVID virus knows no boundaries and as millions become infected quickly there is even more potential for new mutations to occur that could cause international concern.
Here in Canada we have been dependant on vaccine supplies from abroad that were slow to arrive and the process was complicated by international bartering. In the past month, things have ramped up well and we are projected to receive increased supplies over the next few weeks. In Ontario we are now vaccinating at a per-population rate that is second only to the U.S. That will certainly help us to achieve a lower rate of infection if we can continue to disperse vaccines at this pace and a significant proportion of our population accesses them. The Globe and Mail reported today that if our vaccine supplies arrive as scheduled, all eligible Canadians could be fully vaccinated by the end of July!
What can we learn from what we have seen in other countries? It appears that keeping the long-requested restrictions on mingling, shopping, meeting indoors, and traveling combined with aggressive roll-out of vaccination is the key to gaining some control over the virus. In the past week our COVID new case numbers in Canada seem to be plateauing but it is discouraging that they do not seem to be dropping very quickly. In Kingston where over 40% of our population have received one dose of vaccine and have been under a “stay at home” order for the past two weeks, new case numbers are not falling significantly (yet). Our Canadian provincial governments, faced with Health Care systems that are at capacity, have needed to impose increased restrictions. We all have been quite aware what we need to do but many of us are just not following the requested behaviours. We will soon have four vaccines available with age limits dropping almost daily. Vaccine supplies will be coming at a much better rate in May and June. If Canadians accept whatever vaccine they can get soonest there will be more of us who are protected and the virus will have fewer hosts to infect. We are doing pretty well, in fact, with almost 40% of our population having received at least one dose of vaccine. According to the graph below, this puts us about two months behind the UK and three months behind Israel in this regard. So, if we keep the restrictions in place for a while longer, comply with the requests of our Public Health officials and reopen gradually, and if vaccine supplies continue as predicted and are administered as quickly as possible to a willing population we should be able to see great improvement over the next few weeks.

Does it matter which vaccine you get? In the long run, not really. The numbers are sometimes confusing and variable but the bottom line is that they are all effective at significantly reducing infection and all are very effective at preventing severe illness if you do become infected after two doses. Although there is some benefit two weeks after the first dose, this is variable and may not protect quite as well against the Variants of Concern. After one dose only, we are advised to still protect ourselves and others as though we have not had the vaccine yet. The delay of the second dose to complete the vaccination protocol will help our communities to achieve at least partial protection in that vaccines can be distributed to more people as first doses and offering at least partial protection to more people and bring down case numbers. To me, this makes sense. The booster dose, although delayed, will add to that effectiveness.
Significant side effects caused by COVID vaccination are rare. Any medical treatment has the potential for significant adverse effects. Physicians are always weighing the Risk/Benefit ration when we prescribe anything or do any medical procedure. Even low-dose aspirin can, in a small number of patients, cause serious gastrointestinal bleeding. Unfortunately, bad news gains attention so we all learn first about the unlikely exceptions, rather than the rules. The potential for a rare blood clotting disorder (not at all similar to usual blood clotting problems like deep vein thrombosis or pulmonary embolus, by the way) may be real but is extremely rare. The chances of serious consequences of a COVID-19 infection are much greater.
People who choose not to be vaccinated can make that choice but, in doing so, they may be giving up certain opportunities for travel or certain other activities or gatherings that will require a “vaccine passport”. I think that is fair.
Can we look forward, then, to achieving the kind of curve that has happened in Israel and the UK? How will can we achieve that?
We avoid spending time indoors at restaurants, gyms, churches or theatres until the virus is much better controlled. We now know that airborne transmission is part of how this virus spreads so any indoor gatherings without a mask for any period of time puts us at risk for infection, no matter if we are 2 metres away or not so we avoid spending indoors with a group of people.
We avoid travel outside our district or having visitors from outside because this increases the risk of introducing new variants to our community. The MOH at the Kingston, Frontenac, Lennox and Addington Health Unit has repeatedly expressed that most of the surges in virus activity in our district have been initiated by travel in or out of our community.
We continue to wear a mask in stores and many other indoor settings and even outdoors if there are a number of people around and you can not adequately distance. This may be a requirement for some time to come.
We take whatever vaccination we can get soonest. The more of us who are vaccinated, the fewer will be vulnerable to infection and spread it to others. It may be that a third or annual booster is required to keep us safe from new variants (much like annual Influenza shots).
We stay off work and isolate from others as much as possible when we are ill. Our provincial governments must not be too eager to drop the restrictions but follow a slow and graded reopening process.
What might slow down progress? New variants that are more easily spread and/or more virulent may arise spontaneously. Hopefully the vaccines we have and any modifications that ensue will be able to continue to be effective at combating them. We also need a substantial acceptance of complete vaccination to achieve herd immunity. When it comes time to open up again it would be best to do it very gradually. Reopening too quickly was a factor in making this third wave more serious. We also need global cooperation and assist lower income countries because as long as the virus is not contained, spread internationally will occur.
And finally, the Globe and Mail estimates that by the end of July, the country should receive enough doses for all eligible people to be fully vaccinated. When we complete our vaccination we can joyously dance the bhangra like Gurdeep!