
As anticipated, Kingston has seen a blip in COVID-19 cases in the past month. Students returning to post secondary facilities, people traveling outside our district or visiting from other communities, the arrival of cooler weather and more indoor activity, and a generally younger demographic acquiring and sharing the virus all triggered that predictable rise in cases.
Our little wave seems to have peaked – for now at any rate. This might be luck but I like to think it is the result of people within our Health Unit generally being responsible and taking care for themselves and our community. Congratulations and thank you for that.

As of this afternoon we have only five known active cases in our district of over 200,000 people. This is very good news and generally indicates that the virus is under reasonable control in our environs. It’s not the same for some other areas in Ontario including the GTA, Ottawa and even Hamilton where one “fitness studio” has been thought to have been a source for over 74 cases.

Other areas of Canada and around the world are struggling to contain this second wave. Italy, France, and the UK, for example, are all experiencing case numbers that greatly exceed the peaks in March. Fortunately, because of improvements in management and the high number of cases in less vulnerable, younger adults, death rates have not shown the same peaks (although they are rising). The U.S. seems not to have ever escaped their first wave. This week their new case numbers are rivalling the highs seen in July.
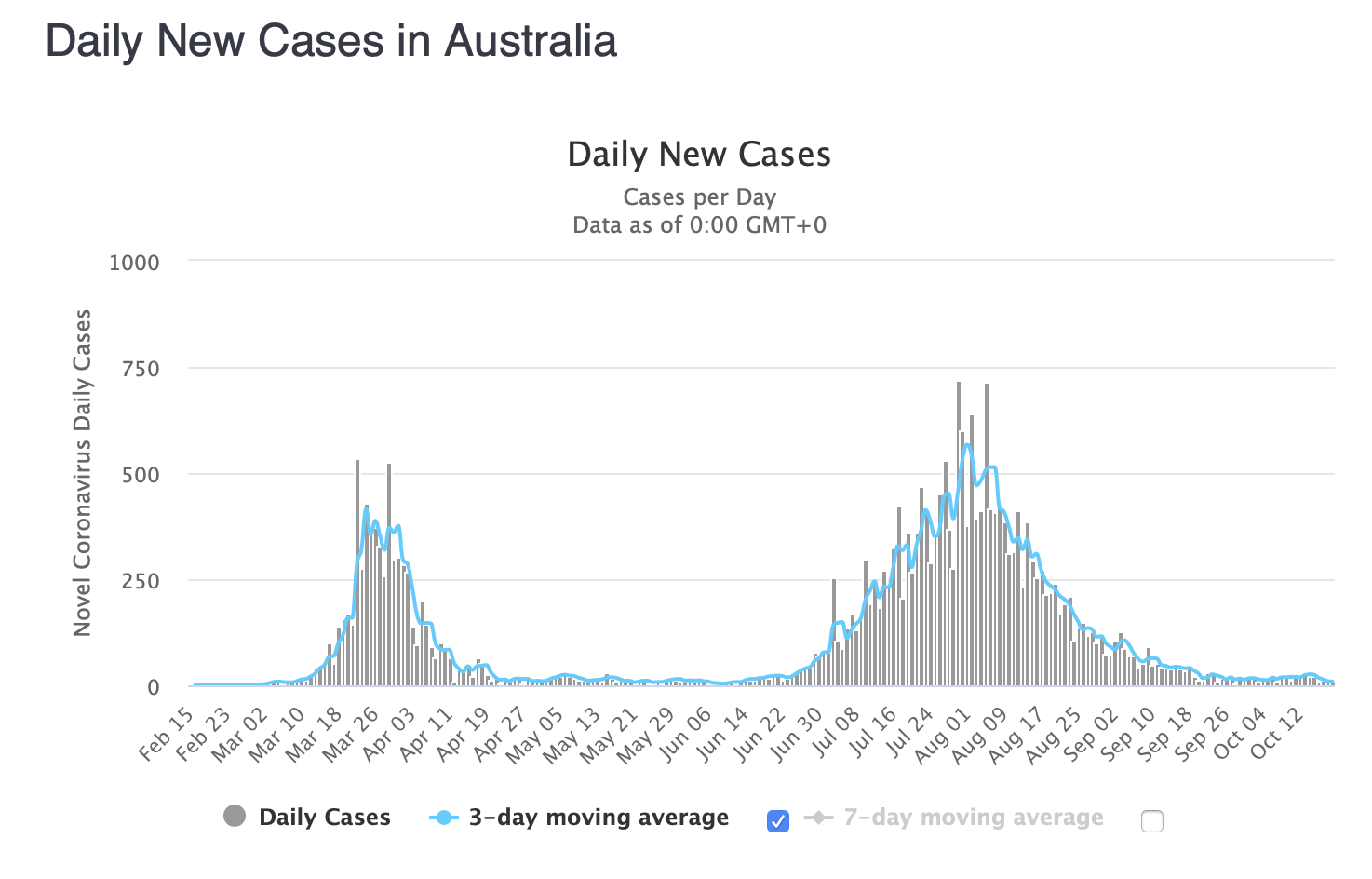
Australia, after seeing very low numbers for months, had a dramatic surge in Melbourne in late July resulting in daily new cases of over 700. They took determined action to reduce spread, including shutting down that district. Today their new case rate for the country was 8.
So, you see, it is possible to keep a lid on this virus but it requires discipline and following the recommendations from our Public Health authorities. These recommendations might vary from district to district depending on the numbers of new cases, whether there is evidence of community spread (ie not from travel outside the district or as a direct close contact of a known case) and whether our health care/hospital resources are being stretched. As far as I can determine, despite our recent Kingston wave, no patients were hospitalized. Since the beginning of the pandemic in March, we have had no cases acquired in our health unit that have required ventilation.
Let’s work on keeping it that way. How can we do that? It’s pretty simple, really.
Wear a mask/face covering when indoors with others in stores, theatres, churches, or any closed space – or even outdoors when social distancing is not possible. Wash hands often.
Keep our social interactions limited to a few close friends and family who we know are also being careful. Avoid indoor gatherings of several people when social distancing will be difficult to maintain.
Avoid traveling outside our community or having friends or family from elsewhere come to visit.
Stay home if we are ill and, if we have symptoms that we think might be COVID-related, get tested and isolate until the test proves negative.
Download the COVID app so we can be notified if we have unwittingly stood beside someone at the grocery store for a few minutes and they have subsequently tested positive.
Get a flu shot. They are now available. I’ve had mine. It won’t prevent COVID-19 but will lessen the circulation of influenza viruses.
We will have to follow these recommendations for the next several months. But eventually this will subside. We are all experiencing COVID fatigue but these inconveniences far outweigh the perils of increased community spread or the necessary economic lockdown that would be precipitated by increasing prevalence. If we are able to keep new cases low, our Health Unit will be able to trace and quarantine patients early. This, too, will limit the spread in the community.
I continue to feel encouraged that management of severely ill COVID-19 patients will continue to improve and that more effective medical management will reduce deaths. A vaccine will be on the horizon soon although it will take a while to dispense it. We may be thwarted from quickly reaching herd immunity by people who decline immunization but eventually those of us who do accept vaccination will help lower the prevalence of virus within our community and this will benefit everyone.
There will soon be a rapid test for the virus and saliva tests will become more common than the usual nasopharyngeal swab. The increased number of testing sites, including in two local pharmacies opened this week for asymptomatic clients, will make it more convenient to be assessed and hopefully lead to earlier detection and isolation of infected people.
We are in a much better place now than we were in March and we have been really fortunate in the KLFA Health Unit to have been less affected than many districts in Canada or worldwide.
Can we hold the line? I hope so. Stay the course.

