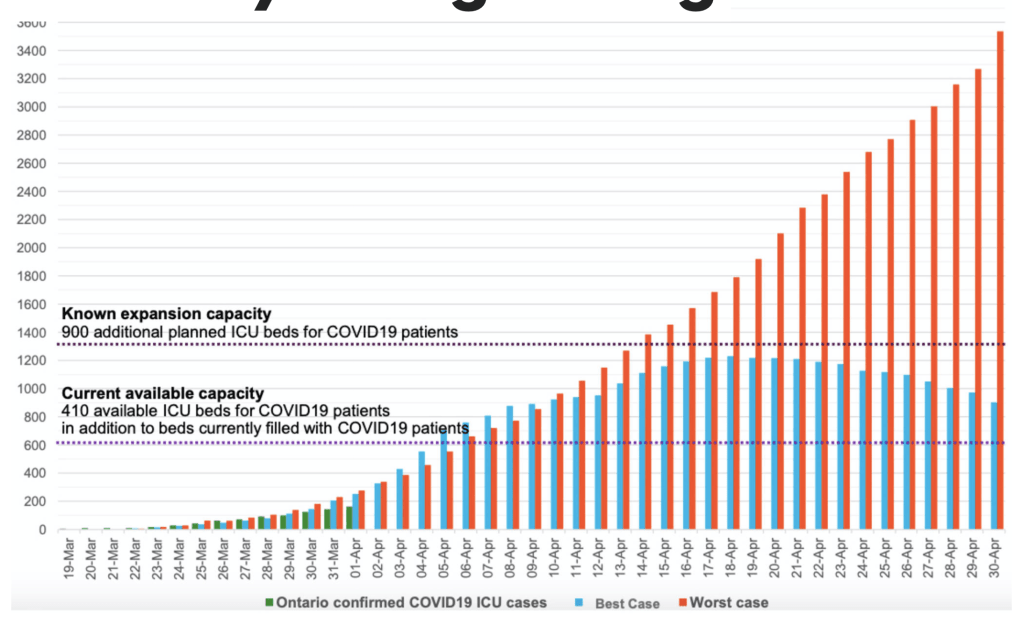
Kingston has remained fortunate that the COVID-19 virus has not caught hold here as it has in some other Canadian communities. Canada’s numbers have plateaued but not dropped significantly in the past week. Ontario’s numbers actually went up a bit last week but today’s count is better. The GTA is the biggest contributor to new Ontario cases. The numbers do bounce around somewhat so looking at the trend (and deaths) gives a better sense of what is happening than daily counts. Canadians have been able to keep the demand on our Health Care facilities manageable and that was the initial aim of all the restrictions requested of us. But there is still risk of clusters of spread and we’ve seen that some folks are being somewhat defiant.
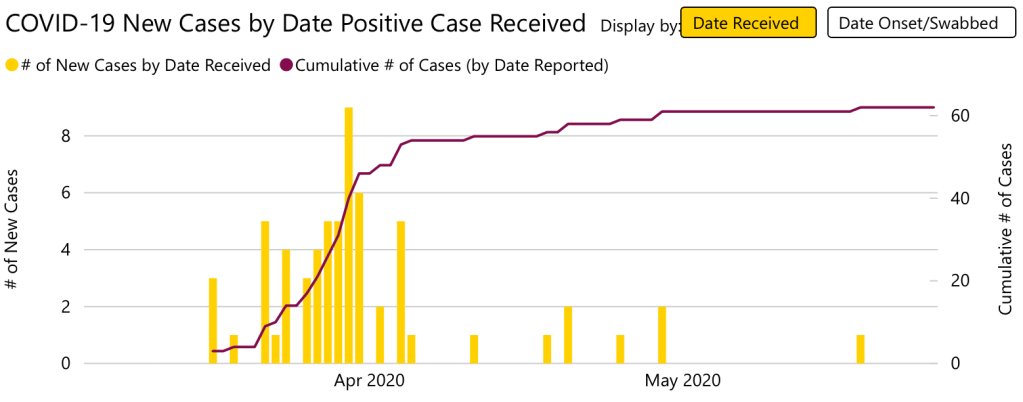
In Kingston, our only new COVID case in the past four weeks has been someone who reportedly went to the Greater Toronto Area and brought it back. I don’t know the exact details but this does point out that Kingston’s greatest risk at the moment is introduction of the virus from people outside our district that we invite in (tourists, relatives) or Kingstonians who travel, don’t adequately physically distance themselves, and then bring COVID-19 home with them. Initially we were asked to STAY HOME, meaning indoors and not going outside for anything other than groceries or something deemed urgent. Most of us complied. It worked. Now the message is still STAY HOME but the definition of “HOME” could be expanded to be within our district. The stats from the KFLA Health Unit for the past month would suggest that picking up COVID-19 in our district from people who have stayed inside our community is negligible.
That is great news. Let’s not get complacent, however. You don’t know who the interloper might be.
We have adjusted to a new social normal already. In general, people are seeming to keep their distance in public places. No one is offended if you veer away from them on the sidewalk. Most people walking together are courteous enough to move to single file to let others pass within a safe distance when the pathway is narrow. I thought today how, in the past few weeks, I have said hello to many more strangers than I did in the past and I’ve been greeted with smiles and responses.
We will adjust to the changes required to keep us safe. I remember, as a child, bouncing around in the back seat of my parents’ car without a seatbelt and how much of an unwelcome restriction it was to have to wear one. Do you recall how restauranteurs and bar owners thought that a no-smoking policy would ruin their business? Think about the changes in airport security that we accept now as normal when virtually none existed only a few years ago.
If you can adjust to standing by your German Shepherd as it takes a dump by the fire hydrant, then bend over to scoop up the poop in a plastic bag that you carry nonchalantly on the rest of your walk, you can certainly adjust to putting on a mask when you go into a grocery store.
There will be other societal changes to which we will acclimatize. Cash will disappear. That trend has already started in many countries but these events will accelerate that movement. For some time, indoor gatherings like theatre or conferences or church will be discouraged. And people will be reluctant to participate, even if they were to occur. Limits to the number of people in a store will be common place. Take out meals will be more comfortable than indoor dining for a while. There will be sanitation changes required to public washrooms. Travel will be cumbersome and awkward.
We will adjust. We have done so to many other societal changes in the past.
Eventually this virus will run its course or become manageable with medical treatment and immunization. In the meantime, we must remain cautious but not scared, compliant with the recommendations made by our Public Health Unit, friendly from a distance and courteous and respectful of others. As a community we can support each other and protect each other. We already have, in fact. Let’s keep that up, Kingston.